
Health-Tech
AI-Assisted Workflow
Safety-Critical UX
AI-assisted triage that speeds
decisions without taking control
away from nurses.
Full app working
My Role
Product Designer, AI
-End to End Design,
-AI Prototyping,
-Vibe Coding, Handoff
Team
2 Product Designers
2 UX Researchers
Tools
Figma Make
Figma
Miro
Github
Overview
The problem in one sentence
Nurses spend up to 15–20 minutes triaging a single patient because clinical data is fragmented
across multiple EHR modules—forcing manual hunting instead of clinical thinking.
Context
Classical hematology referrals range from benign abnormalities to early signs of malignancy.
Triage nurses and hematologists must review fragmented referral notes, labs, and messages to
decide urgency and care disposition—often under tight capacity constraints. Delays and
inconsistencies directly affect patient safety, access to care, and clinician workload.
Goals
Reduce data-gathering time
Unify scattered EHR data into
one workspace so nurses
decide faster.
Improve triage accuracy
Surface key clinical signals
instantly to reduce under-
triage and errors.
Preserve clinician control
AI augments decisions —
nurses always have the final
say.
Opportunity
How might we design an AI-assisted system that reduces cognitive burden while preserving clinician control and trust?
Research
Triage Nurse — Primary User
Who: A registered nurse responsible for reviewing incoming hematology referrals and assigning
urgency tiers before any doctor sees the case.
Pain: Labs, referral notes, imaging, and messages are scattered across multiple EHR modules.
Every review means manually opening tabs, cross-referencing values, and building a mental
model from scratch — under time pressure.
Consequence: High-risk referrals can be delayed. Low-acuity cases consume unnecessary clinic
time. Triage inconsistencies between nurses compound the problem at scale.
Need: A calm, unified workspace that surfaces the most relevant data first and provides
explainable AI support — without removing clinical control.
Doctors — Secondary User
Who: Hematologists who receive and act on the triaged referrals.
Pain: Referrals often arrive incomplete or poorly organized, requiring time-consuming
clarification and re-review before they can decide on care path.
Need: Clear triage logic, visibility into how decisions were made, and confidence that high-risk
cases are escalated appropriately.
Core Pain Points
Fragmented clinical data
Labs, notes, referrals, and
history live in different tabs.
Nurses waste time hunting
instead of deciding.
Complex lab interpretation
Abnormal CBCs, trends over
time, prior transfusions, and
oncology history require
manual cross-checking.
Expertise gap
Due to patient complexity,
nurses need a high level of
expertise — gaps can lead to
under-triage errors.
Though triaging time was an issue, it was not the primary
concern. The primary concern was accuracy of triaging.
Analysis
Research — Plot Twist
We had a chance to speak with hematology physicians from Mayo Clinic. Through direct
conversations and survey-based analysis, we found that though triaging time was an issue, it was
not the primary concern — and to some extent a consequence of the primary problem.
The primary concern was accuracy.
16.3%
Triage errors in a
hospital study of 1,929
patients
59–82%
Nurse triage accuracy
range across studies
19%
Under-triage rate in
structured nurse
settings
17%
Of total triage time lost
to interruptions
Qualitative findings — Why and how?
—
Nurses balance protocol adherence with real-time judgement under pressure. Factors like
patient condition, system workflow, and lack of support influence decisions.
—
Workload and overcrowding are the most frequently reported barriers to quality triage — with
training and technology helping but not eliminating the issue.
—
Under-triage occurred in up to 19% of cases, and inappropriate referrals around 11%, showing structured triage alone can still misclassify urgency without additional support.
Quantitative findings — What happens and how often?
—
In a hospital ED study of 1,929 patients, triage errors occurred in 16.3% of cases, directly linked to higher workload.
—
Nurse triage accuracy ranged between 59% and 82% across studies — variation tied to experience, case mix, and environment.
—
Interruptions contributed to about 17% of total triage time, slowing assessments and increasing error potential.
Design Process
Agentic AI Feature Framework
The system needed to unify data, improve consistency by summarizing complex clinical
information, and surface relevant signals automatically. We mapped two core AI features to the
identified problems:
—
AI-driven clinical
signal
highlighting
— The system scans the EHR and surfaces the most relevant information
making it easier for the nurse to review the triage decision without manually
searching the chart.
—
Supervised
Triaging
A workflow where the AI prepares a triage recommendation from the EHR,
and a triage nurse reviews and approves it.
Design Constraints & Roadblocks
1. Trust barriers around AI in clinical care
Clinicians are skeptical of AI that feels opaque or authoritative.
→ Explicit explanation instead of hidden logic. Clear visual separation via AI watermarks. Neutral
language with tooltips where necessary.
2. Fragmented and inconsistent data
Referral data varies widely in completeness, structure, and quality.
→ High-impact actions gated until essentials are present. Timeline and summary cards prioritized
with badges. Data checklist enforced.
3. Cognitive load in high-volume triage
Triage nurses manage many referrals under pressure, often on small screens.
→ Calm visual hierarchy with limited colors. Progressive disclosure for trends. Visual graphs for high-
value data only.
Vibe Coding — How we built it
"Vibe coding" involves a shift from manual syntax to high-level intent, using AI to bridge the gap
between design and functional code. Tool - Figma make
01 — Intent-based prompting
Describing desired outcomes in natural language
— "Build a medical dashboard that color-codes
patient urgency based on blood count metrics."
02 — Rapid iteration loop
View the AI-generated preview, identify what
feels wrong, and provide conversational
feedback. The AI updates the codebase instantly.
03 — Polishing & Scaffolding
Advanced logic added by prompting specific
behaviors — "On click, open the message modal"
or "Show a loading spinner when data is
fetched."
04 — Deployment
Once the "vibe" and functionality are aligned, the
system is published to a live URL directly from
the tool.
Solution
Feature 1 — For Triage Nurse
Triage Dashboard
Workload overview with urgency cues, filters, and recent activity for fast re-entry. Roadblock
addressed: fragmented data (#2) and cognitive load (#3).

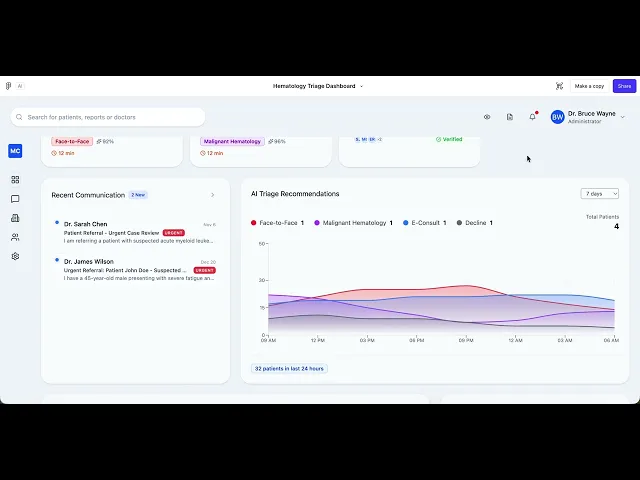
fig 1.0 — Daily To-do's based on urgency
Triage Dashboard Overview: The main workflow view showing active triage tasks in a kanban-style layout. Each patient card displays the AI-generated triage category (Face-to-Face, Malignant Hematology), confidence score, estimated review time, and patient condition at a glance. The right panel shows real-time AI Triage Recommendation trends across all four disposition categories over a 24-hour window.

fig 1.1 — Active patient list
Active Panel list :
Named patient + condition (Iron Deficiency Anemia, Acute Lymphoblastic Leukemia)
AI disposition badge — color-coded with confidence score (92%, 96%) directly on the badge
Estimated review time (12 min) giving workload sense before opening any record
Done column with team member attribution, closing the feedback loop without a separate audit view
Feature 3 — For Triage Nurse
Privacy Mode
Clear AI reasoning with source links and an editable draft triage note — so nurses can validate,
adjust, and own the final decision. Addresses trust barrier (#1).

fig 3.1 —Privacy mode as an admin feature
Feature 4 — For Doctors
Centralized Referral View
Nothing is hidden. Nothing is duplicated. No tab gymnastics. Each referral opens into a single
workspace that brings together everything the doctor needs.

fig 4.1 —Referral communication - Doctors screen
A centralized dashboard that helps administrators and specialists track incoming referrals, current triage status, urgency, and recent communications at a glance. It prioritizes action, not noise, so clinicians spend less time hunting for context and more time dealing with patients who actually need attention.

Before: Doctors hunt across systems to understand one referral.
Now: Each referral opens into a single workspace with the referral note, relevant labs and trends,
documents, and a full clinical timeline — all in one place.
Feature 2 — For Triage Nurse
Unified Patient Workspace
Labs, imaging, documents, and clinical timeline unified in one place. Minimal cognitive load,
maximum signal clarity. Roadblocks addressed: #2, #3.

fig 2.0 — Active patient list
Patient summary :
Named patient + condition (Iron Deficiency Anemia, Acute Lymphoblastic Leukemia)
AI disposition badge — color-coded with confidence score (92%, 96%) directly on the badge
Estimated review time (12 min) giving workload sense before opening any record
Done column with team member attribution, closing the feedback loop without a separate audit view

fig 2.1 — Triage Workflow
Triage Workflow
This view guides clinicians through structured triage decisions by translating referral details, lab values, and clinical context into a clear priority level and recommended care pathway. It standardizes decision-making while still allowing human override, reducing ambiguity in high-stakes cases without pretending doctors are optional.

fig 2.2 — Patient summary
Patient Summary
This feature surfaces a transparent breakdown of why a triage decision was made. It links recommendations to clinical guidelines, highlights key decision factors, and documents reasoning in plain language. The goal is trust and auditability, not blind faith in an algorithm doing mysterious things.
It moves AI from an experimental layer to a practical clinical assistant
Outcomes
While full clinical deployment would require formal trials, projected impact
includes:
↓ Data time
Reduction in data-gathering
time per triage review
↑ Speed
Faster first-pass triage
decisions
↑ Accuracy
Reduced variability between
clinicians
Trust & Adoption
Transparent AI increased acceptance likelihood.
Clear reasoning reduced fear of bias. Clinicians
felt in control, not replaced.
Trust & Adoption
Transparent AI increased acceptance likelihood.
Clear reasoning reduced fear of bias. Clinicians
felt in control, not replaced.
Cognitive Impact
Lower mental load through signal prioritization.
Reduced fatigue from fragmented data across
tabs and systems.
Efficiency
Reduction in data-gathering time. Faster first-
pass triage decisions. More referrals processed
per nurse per shift.
Learnings
01
AI adoption is a trust problem, not a technology problem. Explainability and control matter
more than predictive accuracy alone. Clinicians need to see the reasoning, not just the
answer.
02
Cognitive ergonomics is critical in healthcare. Reducing clicks is not enough — you must
reduce mental processing effort. Every pixel decision carries patient safety weight.
03
Designers must anticipate automation bias. Interfaces must encourage critical thinking, not
blind acceptance. The design must make it easy to disagree with the AI.
04
Clinical environments require humility. AI must defer to human expertise and make that
hierarchy explicit in every interaction.
Future Opportunities
—
Integration with live EHR systems
—
Real-world A/B testing of triage accuracy
—
Measuring time-to-decision metrics in production
—
Expanding into other specialty triage workflows
—
Incorporating adaptive learning models
In summary, we made triage by
Shipping with vibe coding
Used intent-based AI prototyping to rapidly
build and iterate a functional clinical triage
system.
Reducing cognitive load
Unified fragmented clinical data into one
workspace, cutting mental overhead from
cross-tab hunting.
Building AI trust
Transparent AI that shows its reasoning and
preserves full clinician control over every final
decision.
Improving accuracy
Surfaced key clinical signals instantly, reducing
variability between clinicians and supporting
better outcomes.

The future of AI in healthcare is not automation — it is
intelligent augmentation.